
Volume 10, Issue 2 (5-2022)
Jorjani Biomed J 2022, 10(2): 1-9 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Salehi O, kheirdeh M, Farkhaie F, noura M, Jamali Fashi R, Rakhshanizadeh A. The Effect of Interval and Continued Trainings with Citrus Aurantium on Pain Threshold and Motor Balance in Elderly Rats. Jorjani Biomed J 2022; 10 (2) :1-9
URL: http://goums.ac.ir/jorjanijournal/article-1-892-en.html
URL: http://goums.ac.ir/jorjanijournal/article-1-892-en.html
Omidreza Salehi 

 1, Mayam Kheirdeh2 , Fatemeh Farkhaie3 , Mehdi Noura4 , Rasoul Jamali Fashi5 , Abdolali Rakhshanizadeh6
1, Mayam Kheirdeh2 , Fatemeh Farkhaie3 , Mehdi Noura4 , Rasoul Jamali Fashi5 , Abdolali Rakhshanizadeh6
1, Mayam Kheirdeh2 , Fatemeh Farkhaie3 , Mehdi Noura4 , Rasoul Jamali Fashi5 , Abdolali Rakhshanizadeh6
1- Department of Physical Education and Sport Sciences, University of Kurdistan, Sanandaj, Iran , omidreza.67salehi@gmail.com
2- Department of Physical Education, Sama Technical and Vocational College, Shiraz Branch, Islamic Azad University, Shiraz, Iran
3- Department of Physical Education and Sport Sciences, Najaf Abad Branch, Islamic Azad University, Najaf Abad, Iran
4- Department of Physical Education and Sport Sciences, Islamic Azad University, Shiraz Branch, Shiraz, Iran
5- Department of Physical Education and Sport Sciences, Sama Technical and Vocational College, Varamin Branch, Islamic Azad University, Varamin, Iran
6- Department of Physical Education and Sport Sciences, Payame Noor University, Iran
2- Department of Physical Education, Sama Technical and Vocational College, Shiraz Branch, Islamic Azad University, Shiraz, Iran
3- Department of Physical Education and Sport Sciences, Najaf Abad Branch, Islamic Azad University, Najaf Abad, Iran
4- Department of Physical Education and Sport Sciences, Islamic Azad University, Shiraz Branch, Shiraz, Iran
5- Department of Physical Education and Sport Sciences, Sama Technical and Vocational College, Varamin Branch, Islamic Azad University, Varamin, Iran
6- Department of Physical Education and Sport Sciences, Payame Noor University, Iran
Keywords: Aging [MeSH], Citrus [MeSH], Exercise [MeSH], Pain Threshold [MeSH], Rotarod Performance Test [MeSH]
Full-Text [PDF 478 kb]
(960 Downloads)
| Abstract (HTML) (3734 Views)

Aphthous stomatitis is a multifactorial disease, the exact cause has not yet been determine
The interaction of exercise training and antioxidant supplements such as Citrus Aurantium has beneficial effects in improving neuromuscular function.
The interaction of exercise training and antioxidant supplements such as Citrus Aurantium has beneficial effects in improving neuromuscular function.
Full-Text: (483 Views)
Highlights
Recent studies have shown that with the growing aging population in the 21st century, the medical community is facing new challenges and complexities in the diagnosis and treatment of aging-related diseases (1, 2). Muscle atrophy is known as sarcopenia during aging, and with increased oxidative stress, deficiency of mitochondrial function in muscle cells, reduced muscle protein synthesis, reduced muscle fiber counts, reduces muscle strength, and reduced quality of life in older people (3).
Researchers believe that motor problems are one of the challenges of old age and there is a significant relationship between disorders of the locomotor system (bones, muscles, and nervous system), the ability to walk, and the need for nursing services. In addition, disorders such as sitting, standing, and walking are known as motor disorders in the elderly and ultimately lead to muscle weakness, decreased balance, pain, and limited joint movement (4).
In addition, aging by decreasing the number of motor neurons, deficiency in the Insulin-Like Growth Factor-1 (IGF-1) signaling pathway, increases circulating cytokines levels and oxidative stress, and in parallel, the number of muscle fibers decreases (5). Increased oxidative stress and inflammatory cytokines have also been associated with chronic pain in the muscles and joints of the elderly, potentially reducing the function and quality of life of the elderly (5, 6). Overall, muscle and neurological disorders increase the risk of falls in older people and cause irreparable damage to them, so a significant number of people in the United States have lost their normal lives (6). As a result, in recent years, the most important factors that increase the risk of falls are sedentary lifestyle, poor mental state, vision problems, hearing problems, high blood pressure, pelvic floor muscle weakness, medication use, and loss of balance (7).
On the other hand, the positive role of physical activity and exercise in reducing the risks of muscle mass loss due to aging has been shown to improve muscle cell metabolism, increase insulin sensitivity, and increase mitochondrial capacity (8). Studies also show that although physical activity improves oxygen uptake, mitochondrial function, dynamic balance, and static balance in the elderly (9), based on the principle of training overload, training performance is linked to increased training intensity, so it seems that acute exercises and intense exercises, even in athletes, are associated with increased levels of active oxygen species, which these factors cause muscle pain by damage to muscle cells (10); In general, although studies have shown that exercises affect the treatment of many diseases and mechanisms have been identified to influence the pathways of exercise in muscle tissue, the action mechanism regarding the type, intensity, and duration on skeletal muscles (that are impaired by sedation and aging) is not fully understood (11).
Given the limited data regarding the effects of exercise on the skeletal muscles of the elderly, recent research by sports scientists has focused on the administration of antioxidants along with exercise. Merry and Ristow (2016) suggested that antioxidant supplementation along with long-term moderate to intense endurance training as well as High-Intensity Interval Training (HIIT) can improve muscular strength and exercise-induced- pain relief through the mechanism of reducing active oxygen species, increasing antioxidant capacity, mitochondrial biogenesis and insulin sensitivity. Citrus Aurantium (CA) is used in the treatment of some diseases (with compounds such as synephrine and flavonoids) because of its antioxidant effects (12). Researchers have shown the antioxidant effects of CA in PC12 neurons damaged by glutamate (13) in patients with Alzheimer's and Parkinson's diseases (14). Also, the anti-nociceptive effects of CA on moderate to severe knee pain (15) as well as reducing inflammatory factors, increasing antioxidant, and anti-apoptotic factors in smooth muscle have been reported (16).
Given the limited information on the type, intensity, and duration of desirable exercise in the elderly skeletal muscles and chronic pain as well as the role of sedentary on muscle weakness and falling in the elderly; it seems that reviewing the effect of training simultaneously with CA administration can provide more information in this area; Therefore, the present study aimed to investigate the effect of eight weeks of Moderate Intensity Continued (MICT) and HIIT with CA consumption on pain threshold and motor balance in elderly rats.
Materials and Methods
Animal preparation
First, due to higher muscle weakness, loss of mineral mass, and higher risk of falls in women than men (17,18), in this experimental study, 49 elderly female rats (over 14 months of age and 270- 320 g average weight) purchased and were kept in Islamic Azad University of Marvdasht branch animal laboratory one week. This study also followed the guidelines of the International Association for the Study of Pain on ethical standards for the investigation of experimental pain in animals.
It is noteworthy that all the ethical principles of working with laboratory animals in this study were carried out based on the Helsinki Agreement and under the supervision of the ethics committee of the Islamic Azad University of Marvdasht. Also, during the study period, rats were kept in standard conditions of a quiet environment with a temperature of 22-24° C, relative humidity of 55-65%, 12-12 hours of the light-dark cycle, and ad libitum access to water and food for rats.
Grouping and drug administration
Subsequently, rats were randomly divided into seven groups including 1) control, 2) MICT, 3) HIIT, 4) MICT + CA, 5) HIIT + CA, 6) CA and 7) sham (normal saline). During eight weeks groups, 2- 5 ran on a treadmill with prescribed intensity and duration as well as groups 4- 6 received daily 300 mg/kg CA peritoneally.
Experimental design
For performing HIIT and MICT protocols, all rats ran on a treadmill for 5 minutes at a speed of 10 m/min for warming up, then the HIIT groups ran on the treadmill for 7 trail (each trial lasted 1 minute with the speed of 31 m/min) with 6 intervals (each interval 1 minute at a speed of 15 m/min) in the first week which gradually increased to 10 trails (each trial lasted 1 minute with the speed of 55 m/min) with 9 intervals (each interval 1 minute with the speed of 25 m/min) in the eighth week (19). Also, the MICT groups ran on the treadmill for 15 minutes at a speed of 20 m/min in the first week which gradually reached 31 minutes at a speed of 25 m/min in the eighth week. At the end of each training session, all rats ran 5 minutes at a speed of 10 m/min for cooling down (16, 20, 21). The CA groups received daily 300 mg/kg CA peritoneally (22).
Behavioral tests
The motor balance test and pain test were evaluated using a rotarod device (18) and hot plate device, respectively (23, 24). The motor balance is measured by using the Rotarod device. It has a rolling rack with a rotating speed range of 0-40 rpm. The rolling rack speed could be adjusted by relocating the device belts. For the animals to become familiar with the device, they were initially placed on the Rotarod rolling rack so that they could learn how to move on it according to the major protocol (10 rpm rotating speed with 7rpm2 velocity). After 30 minutes, we were ready to start the motor balance test. In this study, the speed was considered to be 10 rpm and the velocity was 7rpm2 which was equal to 10-11 rounds per minute. The amount of time that the animal was able to keep its balance and resist the rolling rack’s movement was recorded as its resistance time. The maximum time of investigation for each animal in the test was 300 seconds (23). The pain threshold was measured by using the hot plate device. The hot plate device was set at 52 C and the animal was placed on this hot plate, and the reaction time or time required for the animal to respond to the stimulus was measured in seconds. The reaction time refers to the time when the animal bites its paws or jumps out of a plastic container on a hot plate (24).
Statistical analysis
The Shapiro-Wilk test was used to evaluate the normality of the distribution of findings. Due to the normal distribution of the findings, a one-way analysis of variance was used to examine the differences between the groups, and Tukey's post hoc test in GraphPad Prism 8.3.3 was used to determine the places of differences between the groups (P≤0.05).
Results
The levels of pain threshold and motor balance are presented in Figures 1- 2, respectively. The results showed that there were no significant differences in pain threshold (P=0.99) and motor balance (P=0.25) levels between the control and sham groups.The pain threshold levels in the CA (P=0.001), MICT (P=0.001), HIIT (P=0.003), MICT+CA (P=0.001), and HIIT+CA (P=0.001) groups were significantly higher than the control and sham groups; in the MICT group, the levels were significantly higher than the HIIT group (P=0.006); in the MICT+CA group, the levels were significantly higher than the CA (P=0.001), MICT (P=0.02) and HIIT (P=0.001) groups; also, in the HIIT+CA group, the levels were significantly higher than the CA (P=0.001), MIACT (P=0.001), HIIT (P=0.001) and MICT+CA (P=0.001) groups (Fig. 1).
- Aphthous stomatitis is a multifactorial disease, the exact cause has not yet been determined.
- The interaction of exercise training and antioxidant supplements such as Citrus Aurantium has beneficial effects in improving neuromuscular function.
Recent studies have shown that with the growing aging population in the 21st century, the medical community is facing new challenges and complexities in the diagnosis and treatment of aging-related diseases (1, 2). Muscle atrophy is known as sarcopenia during aging, and with increased oxidative stress, deficiency of mitochondrial function in muscle cells, reduced muscle protein synthesis, reduced muscle fiber counts, reduces muscle strength, and reduced quality of life in older people (3).
Researchers believe that motor problems are one of the challenges of old age and there is a significant relationship between disorders of the locomotor system (bones, muscles, and nervous system), the ability to walk, and the need for nursing services. In addition, disorders such as sitting, standing, and walking are known as motor disorders in the elderly and ultimately lead to muscle weakness, decreased balance, pain, and limited joint movement (4).
In addition, aging by decreasing the number of motor neurons, deficiency in the Insulin-Like Growth Factor-1 (IGF-1) signaling pathway, increases circulating cytokines levels and oxidative stress, and in parallel, the number of muscle fibers decreases (5). Increased oxidative stress and inflammatory cytokines have also been associated with chronic pain in the muscles and joints of the elderly, potentially reducing the function and quality of life of the elderly (5, 6). Overall, muscle and neurological disorders increase the risk of falls in older people and cause irreparable damage to them, so a significant number of people in the United States have lost their normal lives (6). As a result, in recent years, the most important factors that increase the risk of falls are sedentary lifestyle, poor mental state, vision problems, hearing problems, high blood pressure, pelvic floor muscle weakness, medication use, and loss of balance (7).
On the other hand, the positive role of physical activity and exercise in reducing the risks of muscle mass loss due to aging has been shown to improve muscle cell metabolism, increase insulin sensitivity, and increase mitochondrial capacity (8). Studies also show that although physical activity improves oxygen uptake, mitochondrial function, dynamic balance, and static balance in the elderly (9), based on the principle of training overload, training performance is linked to increased training intensity, so it seems that acute exercises and intense exercises, even in athletes, are associated with increased levels of active oxygen species, which these factors cause muscle pain by damage to muscle cells (10); In general, although studies have shown that exercises affect the treatment of many diseases and mechanisms have been identified to influence the pathways of exercise in muscle tissue, the action mechanism regarding the type, intensity, and duration on skeletal muscles (that are impaired by sedation and aging) is not fully understood (11).
Given the limited data regarding the effects of exercise on the skeletal muscles of the elderly, recent research by sports scientists has focused on the administration of antioxidants along with exercise. Merry and Ristow (2016) suggested that antioxidant supplementation along with long-term moderate to intense endurance training as well as High-Intensity Interval Training (HIIT) can improve muscular strength and exercise-induced- pain relief through the mechanism of reducing active oxygen species, increasing antioxidant capacity, mitochondrial biogenesis and insulin sensitivity. Citrus Aurantium (CA) is used in the treatment of some diseases (with compounds such as synephrine and flavonoids) because of its antioxidant effects (12). Researchers have shown the antioxidant effects of CA in PC12 neurons damaged by glutamate (13) in patients with Alzheimer's and Parkinson's diseases (14). Also, the anti-nociceptive effects of CA on moderate to severe knee pain (15) as well as reducing inflammatory factors, increasing antioxidant, and anti-apoptotic factors in smooth muscle have been reported (16).
Given the limited information on the type, intensity, and duration of desirable exercise in the elderly skeletal muscles and chronic pain as well as the role of sedentary on muscle weakness and falling in the elderly; it seems that reviewing the effect of training simultaneously with CA administration can provide more information in this area; Therefore, the present study aimed to investigate the effect of eight weeks of Moderate Intensity Continued (MICT) and HIIT with CA consumption on pain threshold and motor balance in elderly rats.
Materials and Methods
Animal preparation
First, due to higher muscle weakness, loss of mineral mass, and higher risk of falls in women than men (17,18), in this experimental study, 49 elderly female rats (over 14 months of age and 270- 320 g average weight) purchased and were kept in Islamic Azad University of Marvdasht branch animal laboratory one week. This study also followed the guidelines of the International Association for the Study of Pain on ethical standards for the investigation of experimental pain in animals.
It is noteworthy that all the ethical principles of working with laboratory animals in this study were carried out based on the Helsinki Agreement and under the supervision of the ethics committee of the Islamic Azad University of Marvdasht. Also, during the study period, rats were kept in standard conditions of a quiet environment with a temperature of 22-24° C, relative humidity of 55-65%, 12-12 hours of the light-dark cycle, and ad libitum access to water and food for rats.
Grouping and drug administration
Subsequently, rats were randomly divided into seven groups including 1) control, 2) MICT, 3) HIIT, 4) MICT + CA, 5) HIIT + CA, 6) CA and 7) sham (normal saline). During eight weeks groups, 2- 5 ran on a treadmill with prescribed intensity and duration as well as groups 4- 6 received daily 300 mg/kg CA peritoneally.
Experimental design
For performing HIIT and MICT protocols, all rats ran on a treadmill for 5 minutes at a speed of 10 m/min for warming up, then the HIIT groups ran on the treadmill for 7 trail (each trial lasted 1 minute with the speed of 31 m/min) with 6 intervals (each interval 1 minute at a speed of 15 m/min) in the first week which gradually increased to 10 trails (each trial lasted 1 minute with the speed of 55 m/min) with 9 intervals (each interval 1 minute with the speed of 25 m/min) in the eighth week (19). Also, the MICT groups ran on the treadmill for 15 minutes at a speed of 20 m/min in the first week which gradually reached 31 minutes at a speed of 25 m/min in the eighth week. At the end of each training session, all rats ran 5 minutes at a speed of 10 m/min for cooling down (16, 20, 21). The CA groups received daily 300 mg/kg CA peritoneally (22).
Behavioral tests
The motor balance test and pain test were evaluated using a rotarod device (18) and hot plate device, respectively (23, 24). The motor balance is measured by using the Rotarod device. It has a rolling rack with a rotating speed range of 0-40 rpm. The rolling rack speed could be adjusted by relocating the device belts. For the animals to become familiar with the device, they were initially placed on the Rotarod rolling rack so that they could learn how to move on it according to the major protocol (10 rpm rotating speed with 7rpm2 velocity). After 30 minutes, we were ready to start the motor balance test. In this study, the speed was considered to be 10 rpm and the velocity was 7rpm2 which was equal to 10-11 rounds per minute. The amount of time that the animal was able to keep its balance and resist the rolling rack’s movement was recorded as its resistance time. The maximum time of investigation for each animal in the test was 300 seconds (23). The pain threshold was measured by using the hot plate device. The hot plate device was set at 52 C and the animal was placed on this hot plate, and the reaction time or time required for the animal to respond to the stimulus was measured in seconds. The reaction time refers to the time when the animal bites its paws or jumps out of a plastic container on a hot plate (24).
Statistical analysis
The Shapiro-Wilk test was used to evaluate the normality of the distribution of findings. Due to the normal distribution of the findings, a one-way analysis of variance was used to examine the differences between the groups, and Tukey's post hoc test in GraphPad Prism 8.3.3 was used to determine the places of differences between the groups (P≤0.05).
Results
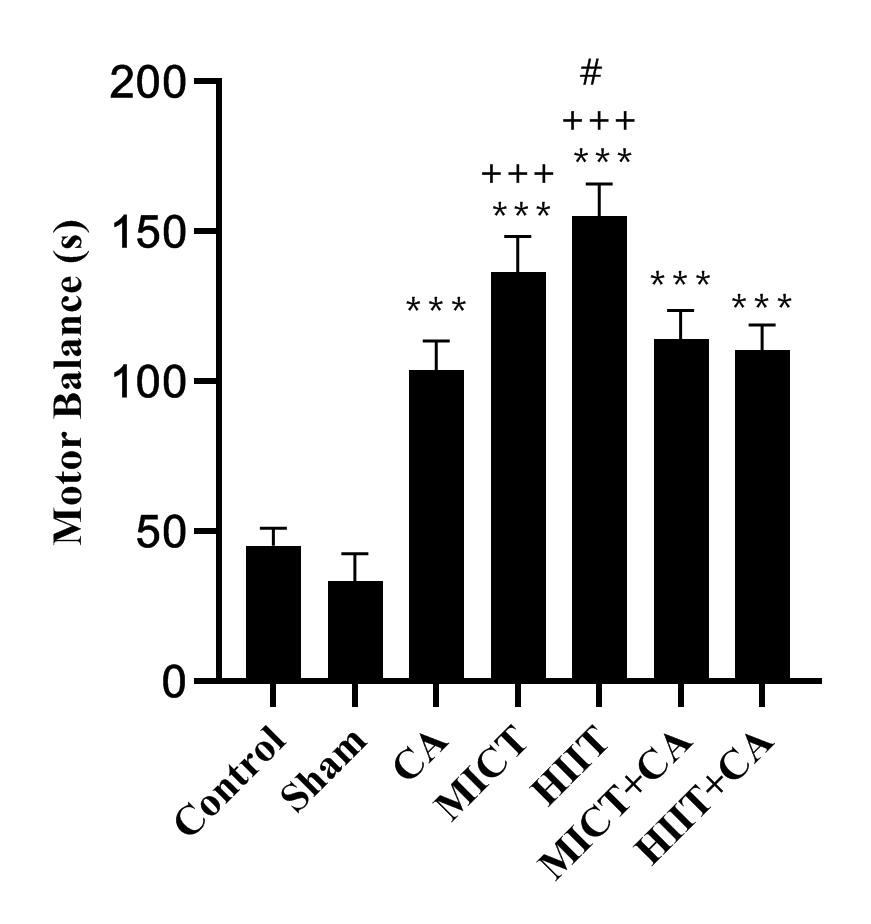
The levels of pain threshold and motor balance are presented in Figures 1- 2, respectively. The results showed that there were no significant differences in pain threshold (P=0.99) and motor balance (P=0.25) levels between the control and sham groups.The pain threshold levels in the CA (P=0.001), MICT (P=0.001), HIIT (P=0.003), MICT+CA (P=0.001), and HIIT+CA (P=0.001) groups were significantly higher than the control and sham groups; in the MICT group, the levels were significantly higher than the HIIT group (P=0.006); in the MICT+CA group, the levels were significantly higher than the CA (P=0.001), MICT (P=0.02) and HIIT (P=0.001) groups; also, in the HIIT+CA group, the levels were significantly higher than the CA (P=0.001), MIACT (P=0.001), HIIT (P=0.001) and MICT+CA (P=0.001) groups (Fig. 1).
Fig 1. Pain threshold in the seven groups of study. Data are presented as mean ± SEM. *** P<0.001 Significant increase compared to the control and sham groups; # # P<0.01 Significant increase compared to the HIIT group; +++ P<0.001 Significant increase compared to the CA and HIIT groups; $$$ P<0.001 Significant increase compared to the MICT and MICT+CA group; & P<0.05 Significant increase compared to the MICT group (CA: Citrus aurantium; MICT: moderate-intensity continued training; HIIT: high interval intensity training)
Fig 2. Motor balance in the seven groups of study. Data are presented as mean ± SEM.
*** P<0.001 Significant increase compared to the control and sham groups; +++ P<0.001 Significant increase compared to the CA, MICT+CA, and HIIT+CA groups; # P<0.05 Significant increase compared to the MICT group (CA: Citrus aurantium; MICT: moderate-intensity continued training; HIIT: high interval intensity training)
*** P<0.001 Significant increase compared to the control and sham groups; +++ P<0.001 Significant increase compared to the CA, MICT+CA, and HIIT+CA groups; # P<0.05 Significant increase compared to the MICT group (CA: Citrus aurantium; MICT: moderate-intensity continued training; HIIT: high interval intensity training)
Discussion
The results showed that HIIT and MICT significantly increased pain threshold and motor balance. Also, MICT compared to HIIT had better effects on the increase of pain threshold; nevertheless, HIIT compared to MICT had better effects on the increase of motor balance. The role of regular exercise in improving aging-related diseases is well known today so researchers have shown that exercise can improve central nervous system metabolism and health. This leads to increased self-esteem and encourages elderly people to exercise; exercise also increases muscle strength, enhances the quality of life, and reduces chronic pain the elderly people (25). Researchers have suggested that aerobic training can increase endorphin levels by the mechanism of increased blood flow, in which endorphin binds to opioid receptors of pain and can reduce pain sensation by blocking the transmission of the pain message to the central nervous system. Another effect of training on pain can be attributed to greater levels of enjoyment of training and physical activity, which can itself be attributed to increased levels of serotonin and dopamine, and reduced fear of movement, which may themselves reduce the stimulation of pain transmitting nerves (26); However, reducing pain and increasing pain tolerance threshold is highly dependent on the initial pain mechanism, as previous studies have suggested that training with the intensity of 50- 60% of maximal heart rate is a safe method for reducing pain in people with chronic pain (27). Polaski et al., (2019) in a meta-analysis study indicated that duration-dependent training has positive effects on pain relief and increased pain tolerance as well as there is a significant relationship between the increase in training intensity and reduction in pain sensation in individuals with chronic pain (28). In another meta-analysis study, Owen et al., (2019) reported that low-intensity aerobic training had more favorable effects on mental health, reduced pain, and increased balance than intense aerobic training and resistance training in elderly people with chronic pain (29).
In the present study, CA had a significant effect on the increase of pain threshold and motor balance. Studies have shown that the arachidonic acid-induced increase in prostaglandins, cyclooxygenase 1 and 2 caused an increase in the sense of pain and inflammation in the human body; On the other hand, various herbal remedies such as aromatherapy and other techniques like oral; appear to reduce pain and relaxation by stimulation of the nervous system neurotransmitters and inhibition of prostaglandins (25). In line with the present study, aromatherapy with CA significantly reduced labor pain (25, 26); also CA administration significantly reduced moderate to severe knee pain (14), inflammatory, antioxidant, and anti-apoptotic factors in smooth muscle (15). Also, it has been noted that CA and citrus family, with their powerful antioxidant effects, reduce oxidative stress in the human body, and by inhibiting caspase- 3 and 8, inhibiting inflammatory and apoptotic factors, can increase nitric oxide, brain-derived neurotrophic factor, activity, and synthesis of tropomyosin, and brain metabolism (27). Although the antioxidant effects of CA have been dose-dependent in previous studies, such that 100 and 300 mg CA extract have a significant effect on the increase of antioxidants in chromium-poisoned lung tissue (28) as well as 1000 mg CA could reduce fat mass, increase strength, and improve quality of life in overweight elderly (29).
In the present study, MICT+CA and HIIT+CA significantly increased pain threshold and motor balance; also MICT+CA and HIIT+CA compared to CA, MICT and HIIT alone had better effects on the increase of pain threshold, so the effects of HIIT+CA were higher than MICT+CA. According to the results of previous studies, it seems that exercises, regardless of the type of training, can improve balance in elderly people through increasing antioxidant factors, muscle protein synthesis, and muscle strength (20), nevertheless, CA (at high doses) increases muscle strength through increasing anti-inflammatory and insulin-like growth factors (15, 27, 30); thus it can be said that exercises and CA can have a synergistic effect on increasing motor balance through separate signaling pathways. On the other hand, a higher-intensity and longer-duration periods of training may have anti-nociceptive effects in the elderly with increased endorphins and neurotransmitters (21), whereas CA has anti-nociceptive effects through reduction of prostaglandins and inhibition of inflammatory factors and cyclooxygenases (25, 31-34). Therefore, it seems that higher effects of HIIT+CA compared to MICT+CA on the increase of pain threshold can be attributed to different signaling pathways.
High-Intensity Interval Training (HIIT) in the initial stages appears to be associated with an increase in reactive oxygen species and an increase in inflammatory agents (35, 36); but in the long run, by adapting, this type of training increases endogenous antioxidants as well as increase total antioxidant capacity, while this type of training increases oxidative stress after each training session (36). However, higher intensity training with antioxidant supplementation can increase the expression of antioxidant enzymes in mitochondria and cell DNA through the same interactive pathways including increasing cyclic AMP, AMPK NRF1 / 2, and PGC1α (19); therefore, it seems that the interactive effect of HIIT and CA in improving pain tolerance threshold is due to the interactive effect of both factors in increasing antioxidant capacity and improving inflammatory factors. However, in justifying the higher effect of CA over HIIT training, it can be stated that although there are conflicting studies on the effect of higher intensity training on oxidative stress and inflammation, CA with isoflavones, synephrine, monoterpene hydrocarbons, adenosine, asparagine, valine, isoleucine, and alanine has a very strong antioxidant effect and no harmful effect of it has been reported even at doses of 1000 and 2000 mg/kg (37).
The lack of measurement of physiological variables of muscle strength and balance as well as the lack of measurement of prostaglandins and antioxidants (to be sure of the results of the present study) are the limitations of the present study. It is therefore suggested that these factors should be evaluated in future studies along with motor balance and pain threshold. Also, since studies have shown that high doses of CA can have more favorable effects, the lack of measurement of this aspect can be another limitation of the present study. It is therefore recommended in future studies that different doses and different administration periods of CA be evaluated.
Conclusion
Although CA, MICT, and HIIT alone can enhance pain threshold and motor balance in elderly rats nevertheless it appears that MICT+CA and HIIT+CA have a better effect on the increase of pain threshold so that the effects of HIIT+CA can be higher than MICT+CA.
Acknowledgments
The authors of this study would like to express their heartiest thanks and gratitude to the research deputy of the Research Center of the Islamic Azad University of Marvdasht.
Conflicts of interest
The authors declare no relevant conflicts of interest or financial relationships.
Funding support
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The results showed that HIIT and MICT significantly increased pain threshold and motor balance. Also, MICT compared to HIIT had better effects on the increase of pain threshold; nevertheless, HIIT compared to MICT had better effects on the increase of motor balance. The role of regular exercise in improving aging-related diseases is well known today so researchers have shown that exercise can improve central nervous system metabolism and health. This leads to increased self-esteem and encourages elderly people to exercise; exercise also increases muscle strength, enhances the quality of life, and reduces chronic pain the elderly people (25). Researchers have suggested that aerobic training can increase endorphin levels by the mechanism of increased blood flow, in which endorphin binds to opioid receptors of pain and can reduce pain sensation by blocking the transmission of the pain message to the central nervous system. Another effect of training on pain can be attributed to greater levels of enjoyment of training and physical activity, which can itself be attributed to increased levels of serotonin and dopamine, and reduced fear of movement, which may themselves reduce the stimulation of pain transmitting nerves (26); However, reducing pain and increasing pain tolerance threshold is highly dependent on the initial pain mechanism, as previous studies have suggested that training with the intensity of 50- 60% of maximal heart rate is a safe method for reducing pain in people with chronic pain (27). Polaski et al., (2019) in a meta-analysis study indicated that duration-dependent training has positive effects on pain relief and increased pain tolerance as well as there is a significant relationship between the increase in training intensity and reduction in pain sensation in individuals with chronic pain (28). In another meta-analysis study, Owen et al., (2019) reported that low-intensity aerobic training had more favorable effects on mental health, reduced pain, and increased balance than intense aerobic training and resistance training in elderly people with chronic pain (29).
In the present study, CA had a significant effect on the increase of pain threshold and motor balance. Studies have shown that the arachidonic acid-induced increase in prostaglandins, cyclooxygenase 1 and 2 caused an increase in the sense of pain and inflammation in the human body; On the other hand, various herbal remedies such as aromatherapy and other techniques like oral; appear to reduce pain and relaxation by stimulation of the nervous system neurotransmitters and inhibition of prostaglandins (25). In line with the present study, aromatherapy with CA significantly reduced labor pain (25, 26); also CA administration significantly reduced moderate to severe knee pain (14), inflammatory, antioxidant, and anti-apoptotic factors in smooth muscle (15). Also, it has been noted that CA and citrus family, with their powerful antioxidant effects, reduce oxidative stress in the human body, and by inhibiting caspase- 3 and 8, inhibiting inflammatory and apoptotic factors, can increase nitric oxide, brain-derived neurotrophic factor, activity, and synthesis of tropomyosin, and brain metabolism (27). Although the antioxidant effects of CA have been dose-dependent in previous studies, such that 100 and 300 mg CA extract have a significant effect on the increase of antioxidants in chromium-poisoned lung tissue (28) as well as 1000 mg CA could reduce fat mass, increase strength, and improve quality of life in overweight elderly (29).
In the present study, MICT+CA and HIIT+CA significantly increased pain threshold and motor balance; also MICT+CA and HIIT+CA compared to CA, MICT and HIIT alone had better effects on the increase of pain threshold, so the effects of HIIT+CA were higher than MICT+CA. According to the results of previous studies, it seems that exercises, regardless of the type of training, can improve balance in elderly people through increasing antioxidant factors, muscle protein synthesis, and muscle strength (20), nevertheless, CA (at high doses) increases muscle strength through increasing anti-inflammatory and insulin-like growth factors (15, 27, 30); thus it can be said that exercises and CA can have a synergistic effect on increasing motor balance through separate signaling pathways. On the other hand, a higher-intensity and longer-duration periods of training may have anti-nociceptive effects in the elderly with increased endorphins and neurotransmitters (21), whereas CA has anti-nociceptive effects through reduction of prostaglandins and inhibition of inflammatory factors and cyclooxygenases (25, 31-34). Therefore, it seems that higher effects of HIIT+CA compared to MICT+CA on the increase of pain threshold can be attributed to different signaling pathways.
High-Intensity Interval Training (HIIT) in the initial stages appears to be associated with an increase in reactive oxygen species and an increase in inflammatory agents (35, 36); but in the long run, by adapting, this type of training increases endogenous antioxidants as well as increase total antioxidant capacity, while this type of training increases oxidative stress after each training session (36). However, higher intensity training with antioxidant supplementation can increase the expression of antioxidant enzymes in mitochondria and cell DNA through the same interactive pathways including increasing cyclic AMP, AMPK NRF1 / 2, and PGC1α (19); therefore, it seems that the interactive effect of HIIT and CA in improving pain tolerance threshold is due to the interactive effect of both factors in increasing antioxidant capacity and improving inflammatory factors. However, in justifying the higher effect of CA over HIIT training, it can be stated that although there are conflicting studies on the effect of higher intensity training on oxidative stress and inflammation, CA with isoflavones, synephrine, monoterpene hydrocarbons, adenosine, asparagine, valine, isoleucine, and alanine has a very strong antioxidant effect and no harmful effect of it has been reported even at doses of 1000 and 2000 mg/kg (37).
The lack of measurement of physiological variables of muscle strength and balance as well as the lack of measurement of prostaglandins and antioxidants (to be sure of the results of the present study) are the limitations of the present study. It is therefore suggested that these factors should be evaluated in future studies along with motor balance and pain threshold. Also, since studies have shown that high doses of CA can have more favorable effects, the lack of measurement of this aspect can be another limitation of the present study. It is therefore recommended in future studies that different doses and different administration periods of CA be evaluated.
Conclusion
Although CA, MICT, and HIIT alone can enhance pain threshold and motor balance in elderly rats nevertheless it appears that MICT+CA and HIIT+CA have a better effect on the increase of pain threshold so that the effects of HIIT+CA can be higher than MICT+CA.
Acknowledgments
The authors of this study would like to express their heartiest thanks and gratitude to the research deputy of the Research Center of the Islamic Azad University of Marvdasht.
Conflicts of interest
The authors declare no relevant conflicts of interest or financial relationships.
Funding support
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Type of Article: Original article |
Subject:
Health
Received: 2022/02/24 | Accepted: 2022/05/7 | Published: 2022/05/22
Received: 2022/02/24 | Accepted: 2022/05/7 | Published: 2022/05/22
References
1. Wilkinson DJ, Piasecki M, Atherton PJ. The age-related loss of skeletal muscle mass and function: Measurement and physiology of muscle fibre atrophy and muscle fibre loss in humans. Ageing Res Rev. 2018;47:123-32. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
2. Hosseini SA, Zar A, Darakhshandeh M, Salehi OR, Amiri R. The Effect of Volume and Intensity Changes of Exercises on Lipid Profile of Elderly Men. J Gerontol. 2017;1(4):38-46. [view at publisher] [DOI] [Google Scholar]
3. Kadoguchi T, Shimada K, Miyazaki T, Kitamura K, Kunimoto M, Aikawa T, et al. Promotion of oxidative stress is associated with mitochondrial dysfunction and muscle atrophy in aging mice. Geriatr Gerontol Int. 2019; [DOI] [PMID] [Google Scholar]
4. Sadeghimahalli N, Hosseini MA, Rahgozar M, Norouzi Tabrizi K. Locomotive syndrome in the elderly and its risk factors. 2019; [view at publisher] [DOI] [Google Scholar]
5. Aagaard P, Suetta C, Caserotti P, Magnusson SP, Kjær M. Role of the nervous system in sarcopenia and muscle atrophy with aging: strength training as a countermeasure. Scand J Med Sci Sports. 2010;20(1):49-64. [DOI] [PMID] [Google Scholar]
6. Chen D, Cao J, Zhu B, Wang Z, Wang T, Tang J. Baicalin attenuates joint pain and muscle dysfunction by inhibiting muscular oxidative stress in an experimental osteoarthritis rat model. Arch Immunol Ther Exp (Warsz). 2018;66(6):453-61. [view at publisher] [DOI] [PMID] [Google Scholar]
7. Liu Y, Chan JSY, Yan JH. Neuropsychological mechanisms of falls in older adults. Front Aging Neurosci. 2014;6:64. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
8. Distefano G, Goodpaster BH. Effects of exercise and aging on skeletal muscle. Cold Spring Harb Perspect Med. 2018;8(3):a029785. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
9. Papa E V, Dong X, Hassan M. Resistance training for activity limitations in older adults with skeletal muscle function deficits: a systematic review. Clin Interv Aging. 2017;12:955. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
10. Withee ED, Tippens KM, Dehen R, Tibbitts D, Hanes D, Zwickey H. Effects of Methylsulfonylmethane (MSM) on exercise-induced oxidative stress, muscle damage, and pain following a half-marathon: a double-blind, randomized, placebo-controlled trial. J Int Soc Sports Nutr. 2017;14(1):24. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
11. Weihrauch M, Handschin C. Pharmacological targeting of exercise adaptations in skeletal muscle: Benefits and pitfalls. Biochem Pharmacol. 2018;147:211-20. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
12. Merry TL, Ristow M. Do antioxidant supplements interfere with skeletal muscle adaptation to exercise training? J Physiol. 2016;594(18):5135-47. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
13. Hosseini A, Sadeghnia HR, Rajabian A. Protective effects of peel and seed extracts of Citrus aurantium on glutamate-induced cytotoxicity in PC12 cell line. Folia Neuropathol. 2016;54:265-77. [view at publisher] [DOI] [Google Scholar]
14. Braidy N, Behzad S, Habtemariam S, Ahmed T, Daglia M, Mohammad Nabavi S, et al. Neuroprotective effects of citrus Fruit-Derived flavonoids, nobiletin and Tangeretin in Alzheimer's and Parkinson's Disease. CNS Neurol Disord Targets (Formerly Curr Drug Targets-CNS Neurol Disord. 2017;16(4):387-97. [view at publisher] [DOI] [PMID] [Google Scholar]
15. Cairncross L, Magee H, Askham J. A hidden problem: Pain in olde r people Picker Institute Europe. Oxford; 2007.
16. Kim J, Chakraborty S, Jayaprakasha GK, Muthuchamy M, Patil BS. Citrus nomilin down-regulates TNF-α-induced proliferation of aortic smooth muscle cells via apoptosis and inhibition of IκB. Eur J Pharmacol. 2017;811:93-100. [view at publisher] [DOI] [PMID] [Google Scholar]
17. Wei F, Hester AL. Gender difference in falls among adults treated in emergency departments and outpatient clinics. J Gerontol Geriatr Res. 2014;3:152. [view at publisher] [Google Scholar]
18. Gale CR, Cooper C, Aihie Sayer A. Prevalence and risk factors for falls in older men and women: The English Longitudinal Study of Ageing. Age Ageing. 2016;45(6):789-94. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
19. Davari F, Alimanesh Z, Alimanesh Z, Salehi O, Hosseini SA. Effect of training and crocin supplementation on mitochondrial biogenesis and redox-sensitive transcription factors in liver tissue of type 2 diabetic rats. Arch Physiol Biochem. 2020;1-6. [view at publisher] [DOI] [PMID] [Google Scholar]
20. Yazdanparast Chaharmahali B, Azarbayjani MA, Peeri M, Farzanegi Arkhazloo P. The Effect of Moderate and High Intensity Interval Training on Cardiac Apoptosis in the Old Female Rats. Rep Heal Care. 2018;4(1):26-35. [view at publisher] [Google Scholar]
21. He W, Li Y, Liu M, Yu H, Chen Q, Chen Y, et al. Citrus aurantium L. and its flavonoids regulate TNBS-induced inflammatory bowel disease through anti-inflammation and suppressing isolated jejunum contraction. Int J Mol Sci. 2018;19(10):3057. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
22. Hosseini SA. The effects of continued training and high intensity interval training along with Citrus aurantium on aerobic power, heart weight, adipose tissue weight and body weight of elderly rats. Jorjani Biomed J. 2020;8(4):17-25. [view at publisher] [Google Scholar]
23. Mallet PE, Beninger RJ, Flesher SN, Jhamandas K, Boegman RJ. Nucleus basalis lesions: implication of basoamygdaloid cholinergic pathways in memory. Brain Res Bull. 1995;36(1):51-6. [view at publisher] [DOI] [Google Scholar]
24. Lüesse H-G, Schiefer J, Spruenken A, Puls C, Block F, Kosinski CM. Evaluation of R6/2 HD transgenic mice for therapeutic studies in Huntington's disease: behavioral testing and impact of diabetes mellitus. Behav Brain Res. 2001;126(1-2):185-95. [view at publisher] [DOI] [Google Scholar]
25. Patti A, Bianco A, Karsten B, Montalto MA, Battaglia G, Bellafiore M, et al. The effects of physical training without equipment on pain perception and balance in the elderly: A randomized controlled trial. Work. 2017;57(1):23-30. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
26. Gordon R, Bloxham S. A systematic review of the effects of exercise and physical activity on non-specific chronic low back pain. In: Healthcare. Multidisciplinary Digital Publishing Institute; 2016. p. 22. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
27. Ambrose KR, Golightly YM. Physical exercise as non-pharmacological treatment of chronic pain: why and when. Best Pract Res Clin Rheumatol. 2015;29(1):120-30. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
28. Polaski AM, Phelps AL, Kostek MC, Szucs KA, Kolber BJ. Exercise-induced hypoalgesia: A meta-analysis of exercise dosing for the treatment of chronic pain. PLoS One. 2019;14(1). [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
29. Owen PJ, Miller CT, Mundell NL, Verswijveren SJJM, Tagliaferri SD, Brisby H, et al. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br J Sports Med. 2019; [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
30. Namazi M, Akbari SAA, Mojab F, Talebi A, Majd HA, Jannesari S. Effects of citrus aurantium (bitter orange) on the severity of first-stage labor pain. Iran J Pharm Res IJPR. 2014;13(3):1011. [view at publisher] [Google Scholar]
31. Heydari N, Abootalebi M, Tayebi N, Hassanzadeh F, Kasraeian M, Emamghoreishi M, et al. The effect of aromatherapy on mental, physical symptoms, and social functions of females with premenstrual syndrome: A randomized clinical trial. J Fam Med Prim care. 2019;8(9):2990. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
32. Mahmoud AM, Hernandez Bautista RJ, Sandhu MA, Hussein OE. Beneficial effects of citrus flavonoids on cardiovascular and metabolic health. Oxid Med Cell Longev. 2019;2019. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
33. Soudani N, Rafrafi M, Amara I Ben, Hakim A, Troudi A, Zeghal KM, et al. Oxidative stress-related lung dysfunction by chromium (VI): alleviation by Citrus aurantium L. J Physiol Biochem. 2013;69(2):239-53. [view at publisher] [DOI] [PMID] [Google Scholar]
34. Colker CM, Kaiman DS, Torina GC, Perlis T, Street C. Effects of Citrus aurantium extract, caffeine, and St. John's wort on body fat loss, lipid levels, and mood states in overweight healthy adults. Curr Ther Res. 1999;60(3):145-53. [view at publisher] [DOI] [Google Scholar]
35. Thirupathi A, Wang M, Lin JK, Fekete G, István B, Baker JS, et al. Effect of different exercise modalities on oxidative stress: a systematic review. Biomed Res Int. 2021;2021. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
36. Lu Y, Wiltshire HD, Baker JS, Wang Q. Effects of High Intensity Exercise on Oxidative Stress and Antioxidant Status in Untrained Humans: A Systematic Review. Biology (Basel). 2021;10(12):1272. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
37. Deshmukh NS, Stohs SJ, Magar CC, Kale A, Sowmya B. Bitter orange (Citrus aurantium L.) extract subchronic 90-day safety study in rats. Toxicol Reports. 2017;4:598-613. [view at publisher] [DOI] [PMID] [PMCID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
